
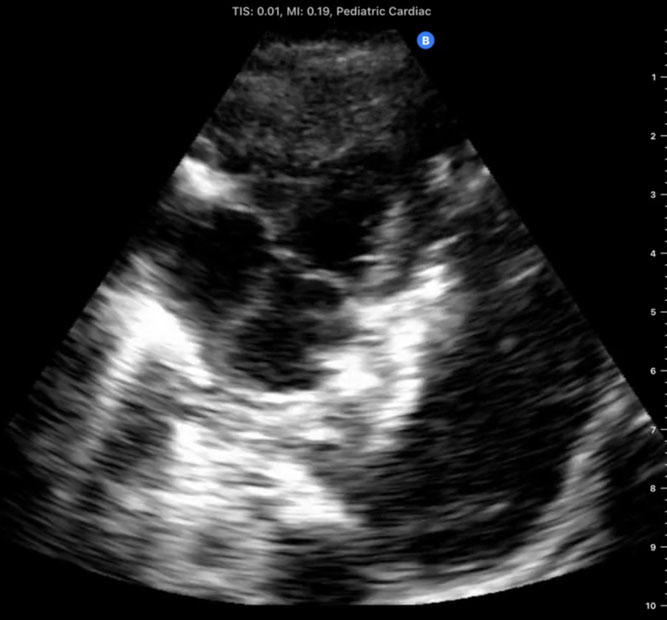
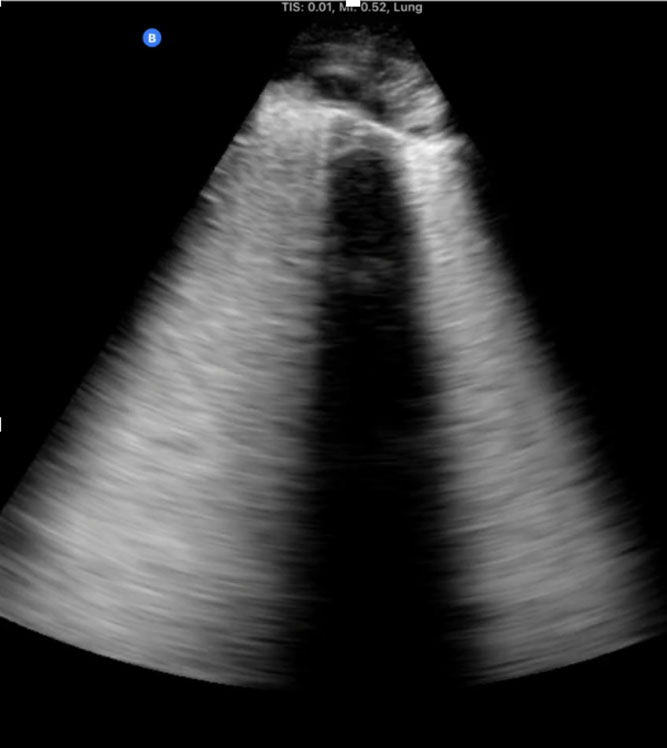
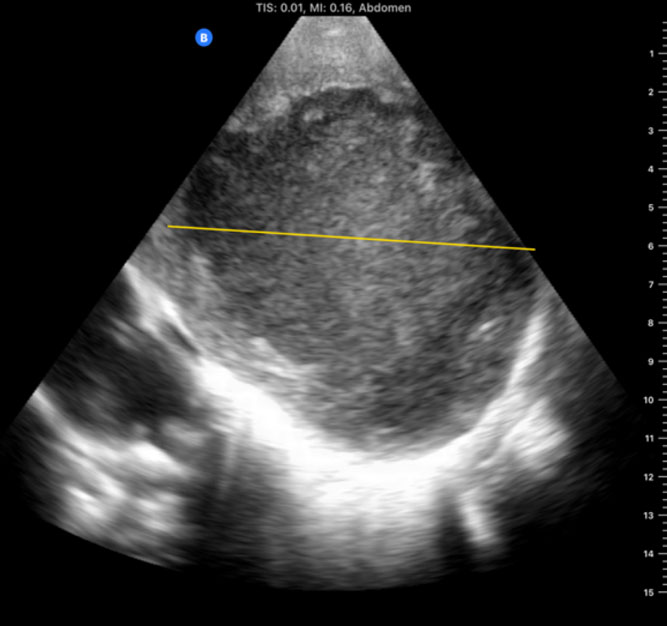
A 6-month-old infant is rushed through the emergency room directly into the Pediatric Intensive Care Unit (PICU) at the Mother and Child Hospital of N'djamena in Chad, Africa. His chest is barely rising with each rapid, shallow breath. A physical examination reveals diminished breath sounds on the left and an oxygen saturation of 80%. Despite being one of the largest hospitals in Chad, it has no portable X-ray machine available. One of our team members on this expedition to Chad brought a personal handheld ultrasound device (iQ, Butterfly Network, Inc, Guilford, CT, USA). Urgently, we performed a point-of-care-ultrasound (PoCUS) evaluation using a left midaxillary and subcostal views, which revealed a huge pleural effusion that was compressing the left lung. Pleurocentes is was guided by the handheld ultrasound, with an almost immediate resolution of the child's respiratory distress. An inspection of the thick fluid drained suggests that the likely cause was tuberculous pleural effusion (TPE).[1]
PoCUS refers to a diagnostic or procedural ultrasound that is performed by a clinician during a patient encounter to help guide the management of the patient.[2] It typically addresses a specific question within a specific context that pertains to the acute care of the patient, such as: Are there signs of pneumothorax? Is there a pleural/pericardial effusion? Are there signs of right heart strain? Is there blood in the abdomen? In high-income countries, PoCUS is utilized by health care professionals of various specialties[3] and has been integrated into the teaching curriculum of many medical schools.[4] Unfortunately, PoCUS is not yet well established in low-income countries (LICs).
Discussion
PoCUS with pocket-size devices is an efficient, safe, and portable imaging modality that is relatively affordable compared to traditional ultrasound machine handheld devices.[5] In low-resource settings (LRS), it has been demonstrated that PoCUS can be utilized for a wide range of indications with substantial impact on clinical decision making.[6] In the past decade, the use of PoCUS by emergency physicians, anesthesiologists, and intensive care specialists has been advocated and implemented with growing success within the perioperative and acute care settings.[7] The most common indications include the assessment of undifferentiated shock, cardiac and pulmonary function, vascular access, aspiration risk, and nerve visualization for regional procedures.[8]
First-hand experience of recent expeditions to low-resource countries (eg, Chad and Sudan), as well as conflict zones such as the Ukrainian front lines following the Russian invasion on February 2022, reveals the substantial clinical utility that PoCUS may have, particularly when other imaging modalities are unavailable. During a recent expedition to Chad, a portable handheld ultrasound device directly assisted in making critical diagnoses and performing life-saving interventions in several men, women, and children. In total, 12 patients (mean age 14.9 years) were managed with the aid of PoCUS with the most common scenarios being trauma after motor vehicle accidents, respiratory failure, and obstetric complications. The most frequent study types performed were the Extended Focused Assessment with Sonography in Trauma (eFAST), cardiac, and lung studies. Within this group of patients, 2 died within this period (a 13-year-old girl with intra-abdominal perforation who traveled for 5 days to the hospital and a 12-year-old extremely malnourished girl who arrived in severe shock and required immediate CPR), and 2 remained with unknown outcomes but carried grave prognoses. PoCUS directed management in 75% of patients, including pulmonary edema in a laboring woman, an amoebic liver abscess diagnosis and ultrasound-guided drainage in a 3-year-old girl, a diagnosis of large pericardial effusion in a 10-month-old boy with Trisomy 21, and the diagnosis of intracranial hypertension using ocular ultrasound in an unconscious 13-year-old involved in a car accident as a pedestrian, suggesting intracranial bleeding.
Several innovative programs in LRS have reported improved clinical outcomes with the use of PoCUS, in Uganda, PoCUS identified significant findings in 70% of patients, changing management in 87% of them. In rural Zambia and Malawi, PoCUS was used for various obstetric indications, including the assessment of fetal presentation and heart rate, placental location, number of gestations, and gestational age. In South Africa, the eFAST exam was utilized for blunt and penetrating trauma victims.[9] In conflict zones and even during combat, it has been demonstrated that PoCUS in the hands of trained clinicians has the potential to improve diagnostic accuracy and ultimately care of the war fighter.[10,11] Outcomes reported in these studies usually involve the ability of PoCUS to positively change clinical management. In a literature review by Abrokwa et al.,[12] PoCUS changed management in 29–81.3% of patients. Despite this wide range, which most probably stems from a heterogeneous population of patients and indications, it is evident that in a significant proportion of patients, this tool significantly advances patient care and improves patient outcomes.[13] As a result of these promising outcomes, efforts to establish more formal longitudinal fellowship initiatives were recently described.[14]
Considering the versatility and the increasing affordability of handheld ultrasound devices, together with the World Health Organization (WHO) estimation that 60% of the world's population does not have access to basic X-ray, computed tomography (CT) scanners, or other imaging tools, it seems worthwhile to promote this low-cost high-yield technology in LRS.[15,16] Nowadays, handheld, smartphone-size machines capable of imaging superficial (vascular, pleura) and deep (cardiac, abdomen) anatomical structures are sold for less than CAD $4000.[17] Additionally, since PoCUS answers focused diagnostic questions, using easily employed techniques, it is relatively simple to acquire PoCUS skills, with studies demonstrating that effective and accurate scans can be performed even after as little as 3 hours of teaching and 5 hours of hands-on training.[18,19]
Barriers to Widespread Use of PoCUS in Low-Resource Areas: Funding for Initial Ultrasound Devices Purchase and Long-Term Maintenance
Even though handheld portable ultrasound devices are more affordable than traditional ultrasound machines, it must be emphasized that affordability is a relative term. While $4000 may be affordable to a foreign physician or organization, this is not the case for a physician in Chad (and likely across other LRS countries). According to Dr Mahamat Nour, the Director (and coauthor) of the Mother and Child Hospital of N'djamena, the average income of a physician in Chad is approximately $850 per month before tax deduction, making the acquisition of a single device the equivalent of a yearly physician salary, rendering it impractical. On a hospital level, while every funding request is directed to the Chadian Ministry of Health by the hospital director for consideration, much more basic needs are in desperate shortage and are therefore more prioritized.
Another crucial yet often overlooked consideration in implementing a successful PoCUS program in LRS is the limited availability of maintenance, repair, and quality assurance of the devices.[20,21] Not only does it involve high costs to maintain this equipment, but also a specialized expertise of necessary personnel that traditional radiologists rely on is required.[22,23] Predicting and planning for potential issues such as broken probe cords, melted charging stations, computer viruses in tablets, ongoing ultrasound gel supply, or even theft of these high-value/ultra-portable devices, are crucial, as failure to do so may set an otherwise promising program to failure.[24,25]
Overall, these economic circumstances leave these crucial steps of initial purchase and longitudinal maintenance in the hands of foreign organizations, requiring local and foreign physicians involved in these activities to act to raise awareness among potential stakeholders. While fundraising practices are beyond the scope of this manuscript, it is imperative to point out that beyond media campaigns[26] and lectures,[27] medical journals play a significant part in distributing these needs and potential interventions, inspiring a targeted and relevant population.
Longitudinal Training
Had it merely been a matter of 1-time funding and basic training, projects which foreign organizations and stakeholders more easily undertake, probes would probably be dispersed and utilized more in LRS. In a study by Maw et al.[28] regarding stakeholder perceptions of PoCUS in resource-limited settings, the authors state that the most significant barriers to a wide implementation of PoCUS are the time and cost required for ongoing longitudinal training. Indeed, maintenance and acquisition of new PoCUS skills under direct guidance require a long-term investment of time and money. In another recently published study of stakeholders' perspectives regarding the implementation of ultrasound guided thoracentesis in Zimbabwe and Nepal, the main themes that emerged were limited access to equipment and training, as well as skepticism regarding the feasibility of an online training approach.[22] As an example, based on data from the organization (Israeli Flying Aid [IFA]) that funded the expedition to Chad as well as dozens of other expeditions to low-resource and conflict zones (Syria, Lebanon, Sudan, Haiti, Indonesia, and so forth), the cost of each basic 7-day medical expedition starts at approximately $20,000, with security constraints mandating significant expenditures. Considering that a longitudinal training program led and implemented by foreign physicians at a minimum of twice a year leads to substantial financial investment, creating a significant barrier to initiation is such an undertaking.
What Can Be Done to Overcome These Barriers and Improve PoCUS Accessibility in LRS?
Reflecting on these barriers and considering the local coauthors' prior experiences, we suggest that following the initial purchase of handheld ultrasound devices, the focus be placed on long-term training of a pre-identified small group of local champions, who would then continue to train others in their area. This paradigm would save, to some extent, the longitudinal training expenditure that prevents many stakeholders from initiating such important undertakings.[28] Additionally, working with local champions who will essentially lead and implement maintenance and new skills acquisition among their colleagues, offers the advantage of overcoming previously published logistical, linguistic, and cultural challenges,[29] while empowering local teams by long-term mentorship. Finally, since local champions continuously train new groups of physicians, travel costs of foreign teams are significantly diminished, resulting in potentially more available funds to be invested in the maintenance of equipment.
Pragmatically, we suggest a PoCUS training program for LRS areas that would ideally be adapted by foreign funders and include the following steps:
- Identify and contact local champions of different specialties (eg, emergency and intensive care, anesthesiology). This step relies either on previous experience, shared intelligence, or low-budget "scouting" expeditions to map needs and establish professional connections.
- Initiate purchase of handheld ultrasound devices according to budget and needs. Practically, once a network of local and foreign medical providers is established and needs are carefully considered, the cost of devices and preliminary on-site training is raised employing aforementioned strategies, while, ideally, cooperating with local health officials (eg, local ministry of health).
- Primary intensive on-site training of local champions led by foreign PoCUS experts.
- Construct a long-term program that includes the 3 steps above, led by only local physicians.
- Longitudinal mentorship consisting of hands-on teaching, journal reviews, and PoCUS education sessions. This longitudinal mentorship program will also then be implemented by the local champions with their trainees.
To maintain longitudinal hands-on training, technological developments in this field prove extremely helpful. Today, Tele-Ultrasound[30–32] is being used more often to assist in the medical management of patients in resource-limited settings. Although research is still required, a systematic review that included 12 studies demonstrated that ultrasound images sent to a remote expert are of satisfactory quality and value for clinical diagnosis and management.[33] This tool may very well be used for educational purposes, implementing the same paradigm, to grow local independent leaders.
Conclusion
Overall, medical advances, including but not limited to imaging techniques such as PoCUS, should be incorporated into medical service in low-resource parts of the world, where other measures such as X-ray or computed tomography (CT) scanners may not be available. Specifically in these circumstances, PoCUS is a game-changer, showing great potential to advance medical care.
References
- Porcel JM. Tuberculous pleural effusion. Lung. 2009;187(5):263–270.
- Atkinson P, Bowra J, Lambert M, et al. International Federation for Emergency Medicine point of care ultrasound curriculum. CJEM. 2015;17(2):161–170.
- Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med. 2011;364(8):749–757.
- Russell FM, Herbert A, Ferre RM, et al. Development and implementation of a point of care ultrasound curriculum at a multi-site institution [Internet]. Ultrasound J. 2021;13. Accessed May 11, 2022. doi: 10.1186/s13089-021-00214-w
- Tran TT, Hlaing M, Krause M. Point-of-care ultrasound: applications in low- and middle-income countries. Curr Anesthesiol Rep. 2021;11(1):69–75. doi: 10.1007/s40140-020-00429-y
- Reynolds TA, Amato S, Kulola I, et al. Impact of point-of-care ultrasound on clinical decision-making at an urban emergency department in Tanzania. PLoS One. 2018;13(4):e0194774.
- Byrne M, Singleton M, Kalagara H, Haskins SC. Perioperative point-of-care ultrasound. Adv Anesth. 2021;39:189–213.
- Naji A, Chappidi M, Ahmed A, et al. Perioperative point-of-care ultrasound use by anesthesiologists. Cureus. 2021;13(5):e15217.
- Sippel S, Muruganandan K, Levine A, Shah S. Review article: use of ultrasound in the developing world [Internet]. Int J Emerg Med. 2011;4. Accessed May 12, 2022. doi: 10.1186/1865-1380-4-72
- Savell SC, Baldwin DS, Blessing A, et al. Military use of point of care ultrasound (POCUS). J Spec Oper Med. 2021;21(2):35–42.
- Balasupramanien K, Comat G, Renard A, et al. Ultrasonography performed by military nurses in combat operations: a perspective for the future? J Spec Oper Med. 2022;22(3):65–69.
- Abrokwa SK, Ruby LC, Heuvelings CC, Bélard S. Task shifting for point of care ultrasound in primary healthcare in low- and middle-income countries, a systematic review [Internet]. eClinicalMedicine. 2022;45:101333. Accessed May 12, 2022. doi: 10.1016/j.eclinm.2022.101333
- Weile J, Frederiksen CA, Laursen CB, et al. Point-of-care ultrasound induced changes in management of unselected patients in the emergency department, a prospective single-blinded observational trial [Internet]. Scand J Trauma Resusc Emerg Med. 2020;28. Accessed May 12, 2022. doi: 10.1186/s13049-020-00740-x
- Burleson SL, Pigott DC, Gullett JP, et al. Point-of-care ultrasound in resource-limited settings: the PURLS fellowship. Ultrasound J. 2020;12(1):14. Accessed May 12, 2022.
- Suttels V, Du Toit JD, Fioghé AA, et al. Point-of-care ultrasound for tuberculosis management in Sub-Saharan Africa, a balanced SWOT analysis. Int J Infect Dis. 2022;123:46–51. Accessed November 18, 2022.
- Kizito PM, Bagonza KD, Odakha JA, et al. Diagnostic performance of point of care ultrasound compared to chest X-ray in patients with hypoxia at a teaching hospital emergency department in Uganda. Afr J Emerg Med. 2023;13(2):61–67. Accessed April 11, 2023.
- Handheld Portable Ultrasound Machine [Internet]. Butterfly Store. https://store.butterflynetwork.com/ca/en/. Accessed August 31, 2022.
- Flick D. Bedside Ultrasound Education in Primary Care. J Ultrasound Med. 2016;35(7):1369–1371. doi: 10.7863/ultra.15.08073
- Robertson TE, Levine AR, Verceles AC, et al. Remote tele-mentored ultrasound for non-physician learners using FaceTime: a feasibility study in a low-income country [Internet]. J Crit Care. 2017;40:145–148. Accessed May 12, 2022. doi: 10.1016/j.jcrc.2017.03.028
- Shaddock L, Smith T. Potential for use of portable ultrasound devices in rural and remote settings in Australia and other developed countries: a systematic review. J Multidiscip Healthc. 2022;15:605–625.
- Henwood PC, Mackenzie DC, Rempel JS, et al. A practical guide to self-sustaining point-of-care ultrasound education programs in resource-limited settings. Ann Emerg Med. 2014;64(3):277–285.e2.
- Doran J, Hanna R, Nyagura-Mangori T, et al. Stakeholder perspectives on current determinants of ultrasound-guided thoracentesis in resource-limited settings: a qualitative study. BMJ Open. 2022;12(12):e064638.
- Mollura DJ, Soroosh G, Culp MP. RAD-AID Conference on International Radiology for Developing Countries: gaps, growth, and United Nations Sustainable Development Goals. J Am Coll Radiol. 2017;14(6):841–847.
- Lamprecht H, Lemke G, van Hoving D, et al. Poor return on investment: investigating the barriers that cause low credentialing yields in a resource-limited clinical ultrasound training programme [Internet]. Int J Emerg Med. 2018;11(1). doi: 10.1186/s12245-018-0168-9
- Shah S, Bellows BA, Adedipe AA, et al. Perceived barriers in the use of ultrasound in developing countries [Internet]. Crit Ultrasound J. 2015;7(1). doi: 10.1186/s13089-015-0028-2
- Articles [Internet]. Israeli Flying Aid. Published 2014. Accessed September 22, 2022. https://ifaid.org/ifa-in-the-media/articles-israeli-flying-aid/
- DARA 2022 AGM Registration [Internet]. Google Docs. Accessed September 22, 2022. https://docs.google.com/forms/d/e/1FAIpQLSelyu0DFkKnXdAoT1xP7c0JbrmwJrV54moqN-eSz9GyapdGZA/viewform
- Maw AM, Galvin B, Henri R, et al. Stakeholder perceptions of point-of-care ultrasound implementation in resource-limited settings [Internet]. Diagnostics (Basel). 2019;9(4). doi: 10.3390/diagnostics9040153
- Bauer I. More harm than good? The questionable ethics of medical volunteering and international student placements [Internet]. Trop Dis Travel Med Vacc. 2017;3. doi: 10.1186/s40794-017-0048-y
- Gibson LE, Low SA, Bittner EA, Chang MG. Ultrasound Telediagnosis to Reduce Healthcare Worker Exposure to Coronavirus Disease 2019. Crit Care Explor. 2020;2(6):e0146. doi: 10.1097/CCE.0000000000000146
- Providing healthcare to rural populations with Real Time Remote Telementored Ultrasound [Internet]. University of North Texas Health Science Center, 2022. Accessed November 18, 2022. https://hdl.handle.net/20.500.12503/30862
- Recker F, Höhne E, Damjanovic D, Schäfer VS. Ultrasound in telemedicine: a brief overview. Appl Sci (Basel). 2022;12(3):958.
- Britton N, Miller MA, Safadi S, et al. Tele-ultrasound in resource-limited settings: a systematic review [Internet]. Front Public Health. 2019;7. doi: 10.3389/fpubh.2019.00244